Solving healthcare logistics: strategies for better patient flow
TL;DR:Healthcare supply chain costs make up 30 to 45% of hospital budgets, with significant waste and inefficiency.Poor logistics increase patient length of stay, emergency department crowding, and drain clinical staff hours.Implementing integrated platforms, automation, and leadership alignment can significantly improve logistics performance.
Supply chain costs represent 30 to 45% of hospital operating budgets, yet a significant portion of that spend evaporates through expired inventory, manual processes, and coordination failures that rarely appear on a leadership dashboard. Clinical staff lose 20 to 25% of their working hours to supply management tasks rather than direct patient care. These are not marginal inefficiencies. They are systemic drains that affect patient flow, discharge timing, emergency department capacity, and the financial stability of entire health systems. This article examines the root causes of healthcare logistics challenges, maps the specific bottlenecks that slow patient movement, and presents evidence-based frameworks that administrators can apply to drive measurable improvement.
Table of Contents
- Understanding the scope: Supply chain and cost pressures
- Bottlenecks in patient flow: Where logistics falter
- Hidden complexities: Staff, coordination, and transport challenges
- Disruptions and edge cases: What most logistics plans miss
- Modernizing healthcare logistics: From strategy to real-world application
- Why rethinking healthcare logistics pays off: A leadership perspective
- Take the next step to improve your healthcare logistics
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Costs are rising | Logistics expenses are growing fast and account for up to 45% of hospital budgets. |
| Bottlenecks harm flow | Inefficient logistics cause longer patient stays, ER crowding, and care delays. |
| Hidden complexities matter | Staff confusion and poor coordination quietly erode system performance every day. |
| Disruptions test resilience | Pandemics and disasters reveal gaps that routine logistics planning often misses. |
| Modernization is essential | Strategic frameworks, automation, and staff engagement are key to logistics success. |
Understanding the scope: Supply chain and cost pressures
The financial weight of logistics inefficiencies is no longer a background concern for hospital leadership. Hospital supply expenses reached $146.9B in 2023, representing 10.5% of the average hospital budget and growing at 9% year over year. When you combine that figure with the reality that 30 to 45% of operating budgets flow through supply chain operations, the scale of exposure becomes clear. Even modest improvements in logistics performance translate directly into millions of dollars in recovered value.
Waste compounds the problem. Industry data consistently shows that 20 to 30% of supply inventory is lost to expiration, overstocking, or misplacement before it ever reaches a patient. Manual procurement and tracking processes amplify this waste by creating gaps between actual usage and recorded consumption. The result is a cycle where hospitals over-order to compensate for uncertainty, which drives up carrying costs and accelerates expiration losses.

| Metric | Current benchmark | Impact |
|---|---|---|
| Supply chain share of operating budget | 30 to 45% | Largest non-labor cost category |
| Annual supply expense growth | 9% year over year | Outpaces most revenue growth rates |
| Inventory waste rate | 20 to 30% | Direct financial loss |
| Clinical staff time on supply tasks | 20 to 25% | Reduces direct patient care hours |
The major cost drivers within this environment include expired and wasted inventory, redundant manual ordering processes, fragmented vendor relationships, and a lack of real-time visibility into stock levels across departments. Administrators who want to maximize logistics efficiencies must address these drivers simultaneously rather than in isolation. Patching one area while ignoring another simply shifts the problem rather than resolving it.
Organizations that have moved toward integrated logistics platforms report meaningful reductions in both waste and administrative burden. Standardizing procurement workflows, automating reorder triggers, and streamlining hospital workflows through coordinated systems are the foundational steps that separate high-performing health systems from those still absorbing preventable losses.
Bottlenecks in patient flow: Where logistics falter
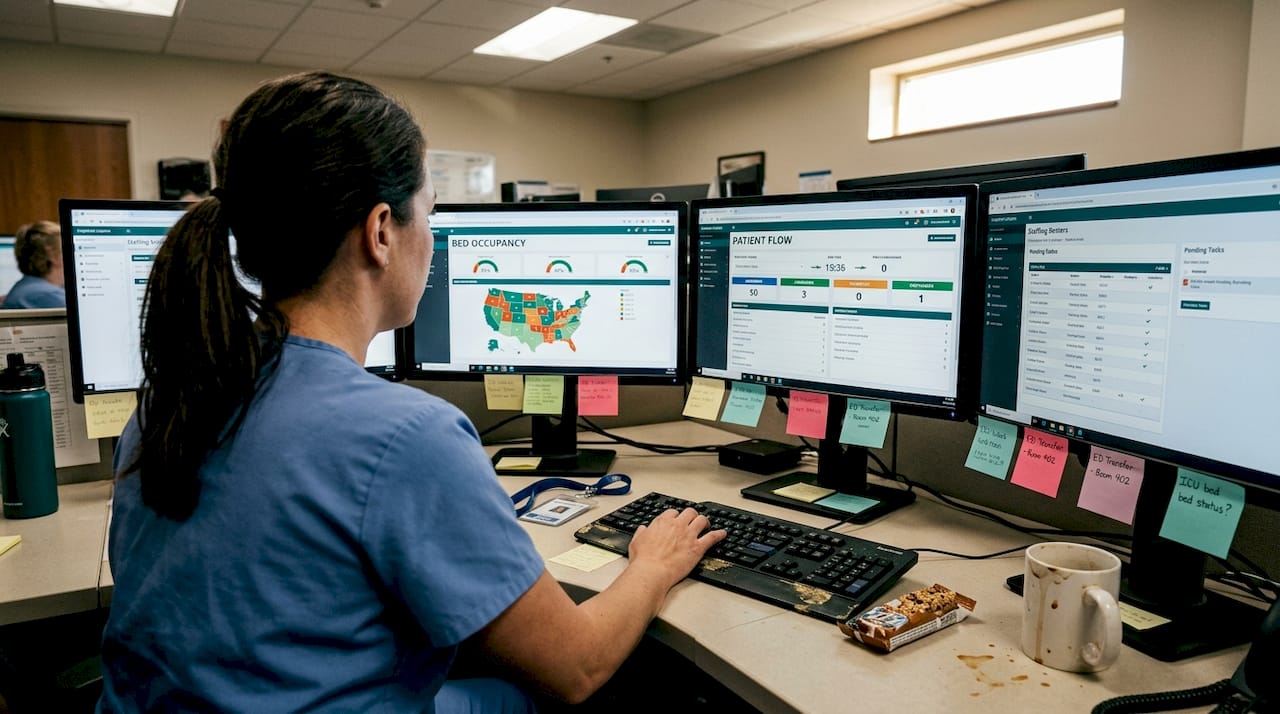
Patient flow is where logistics failures become visible to clinicians, patients, and administrators alike. When a patient cannot move from the emergency department to an inpatient bed because a transport team is unavailable, or when a discharge is delayed because durable medical equipment has not arrived, the consequences ripple across the entire facility. Beds remain occupied, new admissions stall, and emergency department crowding intensifies.
The clinical evidence on this is striking. Patient flow interventions reduce LOS from an average of 11.5 days down to 4.4 days while simultaneously lessening emergency department crowding. That kind of reduction is not achieved through clinical protocol changes alone. It requires logistics infrastructure that supports timely transport, coordinated discharge planning, and real-time communication between departments.
Consider a common scenario. A patient is medically cleared for discharge at 10 a.m. The attending physician has signed the order. But the case manager is waiting on prior authorization from the payer. Transport has not been scheduled. Home health services have not confirmed availability. By the time all parties align, it is mid-afternoon and the bed has been occupied for six additional hours. Multiply that across dozens of daily discharges and the operational impact is severe.

| Process element | Traditional approach | Optimized approach |
|---|---|---|
| Discharge planning initiation | Day of discharge | Admission day |
| Transport scheduling | Manual, reactive | Automated, proactive |
| Payer authorization | Initiated at discharge | Pre-authorized during stay |
| Average LOS | 11.5 days | 4.4 days |
Frontline staff face paradoxes that challenge patient flow success, including gaps between nurse authority and operational responsibility, and tensions between efficiency targets and quality standards. These are not personality conflicts. They are structural misalignments that logistics redesign must account for.
“Structured patient flow logistics reduces average hospital length of stay by more than half, with direct benefits to emergency department capacity and resource utilization.”
Administrators focused on improving patient flow need to map these structural gaps before deploying technology. The tools are only as effective as the processes they automate. Organizations that reduce patient wait times consistently do so by redesigning the coordination layer first.
Hidden complexities: Staff, coordination, and transport challenges
Beneath the visible bottlenecks lies a layer of complexity that most logistics assessments miss entirely. Staff role confusion, departmental silos, and fragmented communication channels create friction that slows every patient movement decision. These hidden complexities are difficult to quantify but easy to observe in facilities where transport delays are routine and discharge coordination feels perpetually reactive.
The key hidden challenges in hospital logistics include:
- Transport coordination gaps: No single owner of the end-to-end transport process means requests fall through the cracks between nursing, transport teams, and external vendors.
- Departmental silos: Supply chain, clinical operations, and patient access teams often operate on separate systems with no shared visibility.
- Staff role ambiguity: Unclear authority over discharge decisions creates delays when multiple stakeholders must align before action is taken.
- Communication lapses: Critical updates about patient status, bed availability, or equipment readiness are transmitted through informal channels that lack accountability.
OR/MS methods for patient transport address these delays directly, recognizing that idle staff and equipment caused by poor transport coordination represent measurable revenue loss. Operations research models can optimize routing, staffing, and scheduling in ways that manual coordination cannot replicate.
“Seven distinct paradoxes challenge patient flow success, including the tension between frontline efficiency and quality, and gaps in nurse authority that prevent timely action.”
The frontline versus managerial perspective gap is one of the most underappreciated barriers to logistics improvement. Managers design processes based on ideal conditions. Frontline staff operate in reality. When these perspectives diverge, workarounds multiply and standardization erodes.
Pro Tip: Establish clear escalation protocols and standardized handoff routines for every patient movement event. When staff know exactly who owns each step and what triggers the next action, ambiguity disappears and delays shrink. This applies equally to patient logistics in SNFs and acute care settings.
Technology platforms that support tech-enhanced appointment logistics and automated dispatch can reduce the coordination burden significantly. Pairing these tools with AI and automation in clinics creates a foundation for consistent, scalable logistics performance.
Disruptions and edge cases: What most logistics plans miss
Standard logistics planning accounts for average conditions. What it rarely accounts for are the edge cases that expose the true fragility of healthcare supply chains and patient flow systems. Pandemic surges, natural disasters, drug shortages, and regulatory delays are not hypothetical risks. They are recurring events that regularly overwhelm facilities with static contingency plans.
The top edge cases that most logistics plans fail to address adequately include:
- Pandemic surge events: Sudden volume spikes require flexible staffing models, surge capacity protocols, and supply chain redundancy that most facilities have not pre-built.
- Cold chain failures: Temperature-sensitive medications and biologics require uninterrupted cold storage. A single refrigeration failure can destroy inventory worth tens of thousands of dollars.
- IV and drug shortages: Over 300 active drug shortages were recorded in 2024, forcing clinicians to substitute medications and administrators to source alternatives under pressure.
- Regulatory and prior authorization delays: Medicare Advantage prior authorization requirements can effectively double patient LOS when discharge planning does not account for payer-specific timelines.
- Post-disaster supply shocks: Regional disasters disrupt vendor networks and transportation infrastructure simultaneously, leaving facilities without reliable resupply channels.
Pro Tip: Replace static disaster plans with dynamic response playbooks that assign decision authority, pre-identify alternative vendors, and include trigger thresholds for escalation. A playbook that requires a committee decision before activating is not a playbook. It is a delay mechanism.
Real-time logistics platforms fill critical gaps here by providing live visibility into inventory levels, transport status, and vendor availability. Facilities that have invested in tools to reduce discharge delays and support disaster response and logistics are measurably better positioned to absorb disruptions without cascading operational failures.
Modernizing healthcare logistics: From strategy to real-world application
The path from logistics dysfunction to operational resilience runs through three interconnected layers: strategic planning, tactical coordination, and operational execution. Each layer requires different tools, different metrics, and different leadership focus. Organizations that treat logistics modernization as a single initiative rather than a layered transformation consistently underdeliver.
Emerging solutions that are proving effective across health systems include:
- Automation of procurement and reorder workflows to eliminate manual intervention and reduce stockout risk
- Standardized patient flow protocols that define ownership, timing, and escalation at every care transition point
- Benchmarking against industry targets for on-time, in-full delivery rates, inventory accuracy, and patient transport times
- Real-time coordination platforms that connect clinical, logistics, and administrative teams on a single data layer
| Framework layer | Focus area | Common pain points addressed |
|---|---|---|
| Strategic | Network design, vendor contracts, capacity planning | Supply fragmentation, cost escalation |
| Tactical | Scheduling, staffing, demand forecasting | Transport delays, discharge bottlenecks |
| Operational | Real-time dispatch, inventory tracking, handoffs | Communication gaps, waste, idle resources |
Research applying stochastic and metaheuristic models to patient flow logistics demonstrates that automation can drive inventory accuracy to 95 to 99% and push on-time, in-full delivery targets to 99%. These are not aspirational benchmarks. They are achievable outcomes for organizations that commit to the full modernization stack.
A thorough patient flow management guide can help administrators understand where their current state sits relative to these benchmarks. Facilities that have addressed oxygen and discharge streamlining as a starting point often find that early wins build the organizational momentum needed for broader transformation.
Why rethinking healthcare logistics pays off: A leadership perspective
Most logistics modernization efforts fail not because the technology is wrong, but because the organizational conditions for adoption are never created. Leadership invests in platforms and workflows while leaving intact the incentive structures, authority gaps, and cultural norms that produced the original dysfunction. The technology runs on top of a broken system and delivers fractional results.
The frontline paradoxes in patient flow research makes this explicit. When nurses lack the authority to act on discharge decisions, no amount of automation resolves the delay. When supply chain and clinical teams are measured on different outcomes, coordination will always be adversarial.
Real improvement comes when logistics is treated as infrastructure, not a support function. That means giving it executive sponsorship, aligning incentives across departments, and designing solutions with input from the staff who will execute them. Understanding patient logistics at this level of depth is what separates organizations that sustain gains from those that revert to old patterns within a year.
Pro Tip: Involve both frontline clinicians and administrative staff in every process redesign session. Their combined perspective surfaces the paradoxes and workarounds that leadership-only design teams consistently miss.
Take the next step to improve your healthcare logistics
The evidence is clear. Logistics inefficiencies cost health systems billions annually, delay patient care, and exhaust clinical staff. The good news is that proven frameworks, real-time platforms, and benchmarked strategies exist to address every layer of this challenge.
VectorCare offers an integrated platform purpose-built for healthcare logistics, from automated transport dispatch to real-time vendor coordination and discharge management. If you are ready to move from reactive firefighting to proactive logistics leadership, start by exploring how to compare logistics solutions that match your organization’s specific needs. Learn why leading health systems are treating logistics as infrastructure and start modernizing logistics with a platform built for scale, compliance, and measurable outcomes.
Frequently asked questions
What is the biggest challenge in healthcare logistics today?
The largest challenge is efficiently managing supply chains and patient flow to reduce waste, cost, and delays, given that supply chain costs represent 30 to 45% of hospital operating budgets with significant embedded waste.
How do logistics problems affect patient care?
Poor logistics directly increases patient wait times, length of stay, and resource delays. Patient flow interventions can cut hospital length of stay from 11.5 to 4.4 days when coordination is properly structured.
What role does technology play in solving logistics issues?
Technology enables real-time coordination, automation, and benchmarking that dramatically improve outcomes. Automation can boost inventory accuracy to 95 to 99% and strengthen supply chain reliability across the full logistics stack.
How can hospitals prepare for unexpected logistics disruptions?
Hospitals should develop flexible response playbooks with pre-assigned decision authority, leverage real-time data systems, and regularly test plans against edge cases. Pandemics and disasters consistently expose the surge planning and real-time visibility gaps that static contingency plans cannot address.
Recommended
- How to Reduce Patient Wait Times Effectively
- Patient Flow Barriers: Impact to Hospital Efficiency and Patient Outcomes | VectorCare
- Maximizing Efficiencies Through Better Patient Logistics | VectorCare
- 6 Ways to Improve Patient Flow Within Healthcare Facilities | VectorCare
- Discover how AI and automation are transforming small clinics into efficient, profitable, and patient-focused practices. Learn practical ways to reduce no-shows, save hours each week, and grow without hiring more staff — all explained in clear, actionable steps designed for real clinic owners.