Patient logistics optimization: 25-38% faster care flow
Hospital administrators who have invested in patient logistics optimization are seeing wait times cut 25-38%, with length-of-stay and throughput improvements following closely behind. Yet most US hospitals still operate with fragmented scheduling, manual bed assignment, and siloed transport coordination that quietly erode revenue, strain staff, and frustrate patients. The scale of avoidable inefficiency is larger than most decision-makers realize, and the evidence for systematic improvement is now robust. This guide covers proven methodologies, real-world benchmarks from leading US health systems, common implementation pitfalls, and a practical roadmap for moving from insight to measurable operational gains.
Table of Contents
- What is patient logistics optimization?
- Core methodologies: From operations research to AI
- Real-world impact: US benchmarks and case studies
- Edge cases and pitfalls: What most hospitals miss
- What works: Practical steps to optimize your patient logistics
- The inside track: Why optimizing patient logistics is harder and more rewarding than it looks
- Next steps: Tools and solutions for patient logistics optimization
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Cut wait times fast | US hospitals using optimized logistics cut patient wait times by up to 38% based on peer-reviewed data. |
| Use proven methods | Operations research, AI, and simulation are the top choices for efficient patient logistics. |
| Pilot, don’t rush | Stepwise pilots with stakeholder input lead to better results than instant organization-wide rollouts. |
| Beware hidden pitfalls | Data gaps and misaligned priorities undermine logistics—plan for edge cases and secure buy-in up front. |
| Technology isn’t enough | Lasting success depends on people, culture, change management, and clear long-term benchmarks. |
What is patient logistics optimization?
With the promise of significant improvements in performance, it’s vital to understand what patient logistics optimization actually entails. At its core, what is patient logistics refers to the coordinated management of every movement a patient makes through a care continuum, from initial transport and bed assignment to intra-facility transfers, discharge, and post-acute follow-up. It also encompasses the resources that support those movements: staff, vehicles, equipment, and information systems.
When logistics are unmanaged or poorly coordinated, the consequences are measurable and costly. Beds sit empty while patients wait in the emergency department. Transport teams idle while nurses make redundant phone calls. Operating rooms start late because pre-op workflows are misaligned. Each gap compounds the next, creating a cascade of delays that affects revenue capture, regulatory performance, and care quality simultaneously.
Patient logistics optimization in US hospitals primarily uses Operations Research (OR) methodologies, alongside AI-driven tools and centralized command centers, to systematically identify and eliminate these inefficiencies. The goal is not simply speed. It is predictable, reliable flow.
Key processes within the scope of patient logistics optimization include:
- Bed management and assignment: Matching patient demand to available capacity in real time
- Patient transport coordination: Scheduling and routing internal and external transport efficiently
- OR and procedure scheduling: Reducing idle time and turnover delays in high-cost care settings
- Discharge planning: Anticipating post-acute needs to prevent bottlenecks at exit
- Resource allocation: Aligning staffing, equipment, and space with predicted patient volume
“Optimal patient logistics is not a single intervention. It is patient logistics as infrastructure, a foundational system that enables every other clinical and operational priority to function at its best.”
Strategic benefits extend beyond operational metrics. Hospitals that optimize logistics report reduced lost revenue from diversion and leakage, higher patient satisfaction scores, and meaningfully better staff retention, because predictable workflows reduce the cognitive and physical burden on frontline teams.
Core methodologies: From operations research to AI
Understanding the bigger picture makes it easier to appreciate the technology and science underpinning effective logistics. The field draws on several distinct but complementary methodologies, each suited to different aspects of the patient flow challenge.
Operations research (OR) provides the mathematical foundation. Linear programming, integer programming, and network flow models allow planners to optimize bed assignments, staff schedules, and transport routing against real constraints. These methods are particularly effective when demand is relatively predictable and constraints are well-defined.
Simulation modeling handles complexity that deterministic models cannot. By running thousands of virtual scenarios, simulation tools reveal how variability in patient arrivals, procedure durations, or transport times propagates through the system. Hospitals use discrete-event simulation to stress-test proposed changes before committing resources.
AI-based dispatch and predictive analytics represent the newest and fastest-growing layer. Machine learning models trained on historical data can forecast admission surges hours in advance, recommend optimal bed placements, and dynamically reroute transport teams in response to real-time conditions. Empirical benchmarks from US hospitals using modeling, simulation, and AI consistently show throughput gains that manual coordination cannot match.
Stochastic and metaheuristic approaches address the inherent unpredictability of healthcare. Genetic algorithms, simulated annealing, and similar techniques find near-optimal solutions in environments where exact optimization is computationally infeasible, such as multi-facility transfer networks or complex OR scheduling problems.
| Method | Best application | Typical gain |
|---|---|---|
| Linear programming | Bed assignment, staffing | 10-20% capacity improvement |
| Simulation modeling | OR scheduling, ED flow | 15-25% wait time reduction |
| AI-driven dispatch | Transport routing, surge prediction | 20-35% efficiency gain |
| Metaheuristic algorithms | Multi-facility transfers | 10-30% leakage reduction |
Critically, better patient logistics efficiencies are not achieved by technology alone. Hybrid human-AI teams consistently outperform pure automation because clinical judgment, local context, and relationship-based coordination remain irreplaceable. Reviewing top transport software options and lowering transport costs are practical starting points for administrators building their technology stack.
The operations research methods literature confirms that no single approach dominates across all settings. Context, data quality, and organizational readiness all shape which methodology delivers the most value.
Pro Tip: Start with a pilot on one high-impact process, such as bed assignment, inter-facility transfer, or OR scheduling, before scaling. A focused pilot generates credible internal evidence, builds staff confidence, and surfaces integration issues before they become system-wide problems.
Real-world impact: US benchmarks and case studies
With the methodological foundation in place, what does successful logistics optimization look like in action? The evidence from leading US health systems is both compelling and specific.
Kaiser Sacramento and University of Louisville Health benchmarks show that centralized transfer centers combined with predictive analytics tools cut wait times by 25-38% and increase overall throughput measurably. These are not marginal gains. At a 500-bed hospital operating near capacity, a 30% reduction in wait times translates directly into additional admissions, reduced diversion hours, and improved emergency department metrics.
Operating room utilization, one of the most financially sensitive metrics in hospital operations, improves by up to 10% when logistics optimization is applied to pre-op and post-op workflows. Leakage, the loss of patients to competing facilities due to slow transfer acceptance or poor follow-up, decreases by as much as 35% in systems that implement structured transfer coordination protocols.

| Metric | Before optimization | After optimization |
|---|---|---|
| Average patient wait time | 90-120 minutes | 55-75 minutes |
| OR utilization rate | 68-72% | 76-80% |
| Transfer acceptance time | 45-60 minutes | 15-25 minutes |
| Patient leakage rate | 18-22% | 12-15% |
| Length of stay (days) | 4.8 | 3.9-4.2 |
The MIT JIT study on just-in-time bed assignment validated 25-37% reductions in patient wait times, reinforcing that the gains seen in health system case studies are reproducible across different hospital types and sizes.
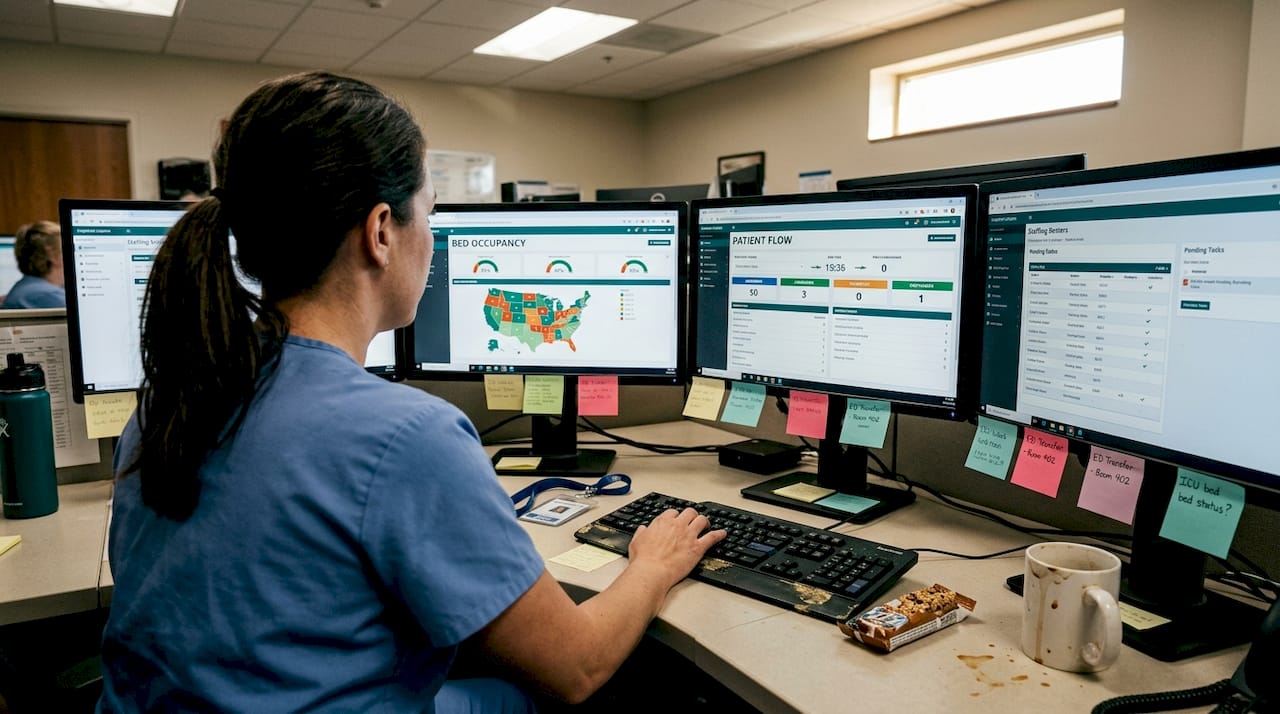
High-performing systems share several consistent practices when it comes to improving patient flow:
- Real-time visibility dashboards accessible to bed management, transport, and clinical teams simultaneously
- Automated alerts that trigger bed cleaning and transport requests without manual handoffs
- Predictive discharge planning that begins at admission, not the morning of discharge
- Regular cross-functional huddles that align logistics teams with clinical priorities
For administrators focused on reducing patient wait times, these benchmarks provide a credible baseline for setting internal performance targets and building the business case for investment.
Edge cases and pitfalls: What most hospitals miss
Results hinge not just on methodology but on anticipating outliers and preparing for common traps. Even well-resourced health systems have encountered costly setbacks when logistics optimization programs failed to account for the full range of operational realities.
Edge case scenarios in logistics optimization include pandemic-level demand surges, high day-to-day variability in patient arrivals, no-show rates that distort scheduling models, and time-dependent transport barriers such as weather, traffic, and staffing shortages. These are not rare events. They are recurring features of hospital operations that any robust logistics system must accommodate.
The most common pitfalls observed across US implementations fall into predictable categories:
- Data silos: When EHR, bed management, and transport systems do not share data in real time, optimization algorithms operate on incomplete information and produce suboptimal recommendations.
- Insufficient staff buy-in: Frontline staff who distrust or misunderstand new workflows will work around them, undermining the system’s effectiveness from day one.
- Rushed rollouts: Compressing timelines to meet budget cycles or executive expectations leads to inadequate testing, poor training, and avoidable failures that damage long-term adoption.
- Local versus system-wide goal conflicts: A department that optimizes its own throughput may inadvertently create bottlenecks downstream. This paradox is one of the most underappreciated challenges in multi-unit hospital logistics.
“The most dangerous optimization is one that appears to work locally while quietly degrading system-wide performance. Measuring only departmental metrics without tracking cross-unit flow is a structural blind spot.”
A change management guide tailored to patient logistics is not optional. It is a prerequisite for sustained results. Securing physician engagement early, before system selection and configuration, dramatically increases the likelihood that clinical workflows will align with logistics protocols rather than conflict with them. Agnostic software for logistics reduces integration risk by connecting existing systems without requiring a full technology replacement.
The hybrid human-AI evidence base is clear: organizations that retain human judgment in the loop, particularly for exception handling and edge cases, achieve more durable results than those that pursue full automation.
Pro Tip: Build change management into the project plan from the first day, not as an afterthought. Assign a dedicated logistics champion from the clinical side who can translate operational logic into clinical language and vice versa.
What works: Practical steps to optimize your patient logistics
Armed with lessons from both standouts and setbacks, here is how to make real improvements in your own hospital. Expert nuances in successful logistics adoption consistently point to a stepwise approach that balances ambition with operational realism.
- Assess current state: Map patient flows across all major pathways, ED, OR, inpatient units, and discharge. Quantify baseline metrics for wait times, transport cycle times, bed turnaround, and leakage.
- Prioritize high-impact areas: Use the assessment data to identify the two or three processes where inefficiency is most costly. The cost of discharge delays is frequently underestimated and often represents the fastest path to measurable ROI.
- Pilot with discipline: Select one process, define success metrics in advance, and run a time-limited pilot with full data capture. Use the results to build internal credibility and refine the approach.
- Implement with cross-functional input: Logistics optimization touches nursing, transport, environmental services, case management, and IT simultaneously. Exclude any one group and the implementation will encounter avoidable resistance.
- Monitor and iterate: Establish a regular cadence of performance review using evidence-based best practices as benchmarks. Logistics systems require ongoing tuning as patient volumes, staffing models, and care protocols evolve.
Key elements of a high-readiness logistics program include:
- Clear, measurable goals aligned with organizational strategy
- Stakeholder buy-in from clinical, operational, and IT leadership
- Integrated data infrastructure that connects scheduling, transport, and bed management
- A feedback loop that surfaces frontline insights to logistics planners regularly
To improve patient flow at scale, health systems must treat logistics not as a back-office function but as a strategic capability that directly enables clinical and financial performance.
The inside track: Why optimizing patient logistics is harder and more rewarding than it looks
With a roadmap in hand, it helps to remember what separates temporary gains from lasting improvement. The honest reality is that most logistics optimization projects that underperform do so not because of technology failures but because of organizational ones.
Clean, integrated data is more valuable than any single algorithm. A sophisticated AI dispatch tool built on fragmented or inconsistently coded data will produce confident but wrong recommendations. Respecting local context matters equally. A bed management protocol that works at an academic medical center may fail at a community hospital with different staffing ratios and patient mix.
Expert nuances and contrasting viewpoints in the literature highlight a risk that rarely appears in vendor presentations: false optimization. A system can move patients faster through one unit while inadvertently creating a new bottleneck two steps downstream, producing metrics that look good in isolation but degrade system-wide performance. This is why why patient logistics is foundational thinking matters so much. Viewing logistics as infrastructure rather than a departmental project forces the cross-unit perspective that prevents these hidden failures.
Culture and communication ultimately determine whether gains persist. Hospitals that sustain improvements invest in ongoing staff education, transparent performance reporting, and leadership accountability for logistics metrics alongside clinical ones. Optimal patient logistics is a never-finished discipline, and that is precisely what makes it so rewarding for the teams committed to it.
Next steps: Tools and solutions for patient logistics optimization
For teams ready to go from insight to implementation, here are valuable resources to get started. The strategies and benchmarks covered in this guide represent what is achievable when health systems treat logistics as a strategic priority rather than an operational afterthought.
Exploring what is patient logistics in greater depth is a strong foundation for any administrator beginning this work. For organizations ready to evaluate technology solutions, the VectorCare patient logistics platform offers an integrated suite of tools covering transport coordination, scheduling optimization, real-time visibility, and AI-driven dispatching, all designed to reduce administrative burden and improve patient outcomes at scale. Teams looking to quantify the opportunity can also review the detailed analysis on maximizing efficiencies through better patient logistics to build a compelling internal business case.
Frequently asked questions
What are the main benefits of patient logistics optimization?
Optimization delivers 15-38% improvements in wait times and length of stay, while also increasing revenue capture, reducing staff burden, and raising patient satisfaction scores across inpatient and transfer settings.
Which tools and methods are used for patient logistics optimization?
Hospitals use OR, AI, simulation, and routing methods in combination, with the most effective programs layering predictive analytics and AI-driven dispatch on top of a solid operations research foundation.
How do leading hospitals achieve logistics gains?
By implementing centralized command centers, predictive analytics, and hybrid human-AI approaches, hospitals have achieved wait time reductions of 25-38%, with the most consistent gains coming from systems that combine technology with strong change management.
What challenges can derail successful logistics optimization?
Data silos, poor buy-in, rushing, and paradoxes between local and system-wide goals are the most frequently cited barriers, and all four are organizational rather than technical in nature.
How should hospitals start optimizing patient logistics?
Begin by assessing current flows, engaging clinical and operational teams, piloting analytics tools on one high-impact process, and scaling up gradually with evidence-based best practices as the benchmark for measuring progress.
Recommended
- How to Reduce Patient Wait Times Effectively
- Patient Flow Barriers: Impact to Hospital Efficiency and Patient Outcomes | VectorCare
- Maximizing Efficiencies Through Better Patient Logistics | VectorCare
- VectorCare - Patient Logistics Platform for Healthcare
- Ghidul pacientului - HELIOS Medical Center - Clinica Medicala Titan - Sector 3
- Streamlining Business Operations for Maximum Efficiency | Gammatica



