Patient flow management tips to cut wait times 38%

TL;DR:Implementing coordinated patient flow strategies can reduce wait times and length of stay by up to 38%.Real-time visibility, standardized processes, and multidisciplinary collaboration are key to sustainable improvement.Advanced technology like AI-powered command centers enables proactive, hospital-wide capacity management.
Structured patient flow management can reduce wait times and length of stay by 25 to 38%, yet most North American health systems still operate with fragmented processes that leave capacity underutilized and patients waiting. For healthcare administrators, this gap represents both a quality risk and a financial liability. Every delayed discharge, mismanaged bed assignment, or uncoordinated handoff compounds downstream pressure across the entire care continuum. This article presents evidence-based strategies, real-world benchmarks, and practical frameworks to help operations and logistics leaders move from reactive firefighting to proactive, systemwide flow optimization.
Table of Contents
- Why patient flow management matters: Real-world impact
- Core strategies for optimizing patient flow
- Discharge optimization: The highest-ROI patient flow lever
- Harnessing technology and analytics for proactive flow management
- Sustaining improvements: Change management, culture, and surge preparedness
- Behind the benchmarks: What most flow management articles miss
- Take patient flow management from knowledge to action
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Measured impact | Strategic patient flow improvements consistently reduce wait times and length of stay by over 25 percent in leading hospitals. |
| Core strategies | Combining real-time tracking, standardized processes, and command centers drives the biggest gains in efficiency and care quality. |
| Discharge optimization | Early, off-peak, and team-based discharge practices can increase throughput by up to 45 percent. |
| Tech-enabled flow | AI-powered analytics and command centers help anticipate surges and manage capacity proactively. |
| Lasting change factors | Sustainable gains depend on hospital-wide coordination, multidisciplinary teams, and strong change management, not just new technology. |
Why patient flow management matters: Real-world impact
Flow bottlenecks are not just a patient experience problem. They drive up length of stay (LoS), inflate cost per episode, and erode staff morale. When beds are occupied by patients awaiting discharge, incoming admissions stack up in the emergency department (ED), creating a cascade that affects every unit in the facility. The financial and clinical consequences are measurable and significant.
Leading North American health systems have demonstrated what is possible when flow management becomes a strategic priority. Kaiser Permanente reduced ED wait times by 38% through coordinated throughput initiatives that aligned bed management, staffing, and real-time data. RWJBarnabas Health achieved a 37% faster admission-to-bed time by redesigning its ED patient flow transformation initiative with cross-functional teams.
| Metric | Before optimization | After optimization |
|---|---|---|
| ED wait time | Baseline | 38% reduction (Kaiser Permanente) |
| Admission-to-bed time | Baseline | 37% faster (RWJBarnabas) |
| Length of stay | Baseline | Up to 25% reduction |
| Patient satisfaction scores | Below benchmark | Measurably improved |
The data makes a clear case. Improving patient flow is not a quality initiative running parallel to operations. It is the operational strategy. Organizations that treat flow as a core performance lever consistently outperform peers on cost, throughput, and patient satisfaction strategies. The ability to reduce patient wait times at scale requires more than individual unit improvements. It demands coordinated, hospital-wide commitment.
Core strategies for optimizing patient flow
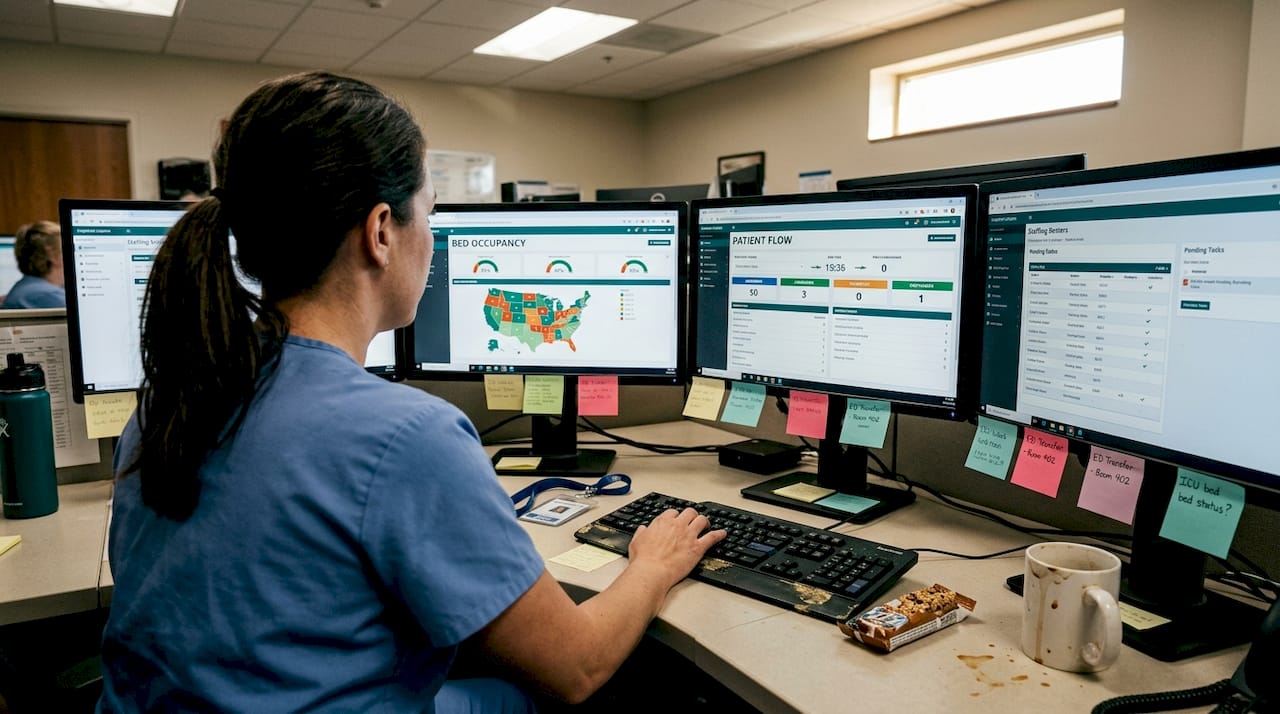
Practical flow improvement rests on four interconnected pillars: real-time visibility, standardized processes, prioritization models, and systemwide oversight. Real-time tracking, bed management, and triage systems are consistently identified as central to sustained improvement across high-performing hospitals.
Real-time bed management gives charge nurses and administrators an accurate, live picture of capacity, pending discharges, and incoming transfers. Without this visibility, decisions are made on outdated information, which creates delays that compound quickly. Pairing bed management tools with structured triage models allows staff to prioritize patient placement based on acuity rather than availability alone.
Standardized handoffs reduce the communication failures that account for a disproportionate share of flow breakdowns. Lean process principles, including value-stream mapping and waste elimination, help teams identify where time is lost between care transitions. Addressing patient flow barriers at the handoff level often produces faster results than investing in new technology without fixing underlying process gaps.
Pro Tip: Before deploying any new flow tool, map your current state process from ED arrival to discharge. Identify the three longest wait intervals. Those are your highest-value targets for workflow streamlining.
A practical sequence for implementation:
- Conduct a current-state flow audit across ED, inpatient, and discharge units.
- Identify the top three bottlenecks by average delay duration.
- Pilot a standardized handoff protocol in the highest-volume unit.
- Deploy real-time bed tracking and integrate with your EHR system.
- Establish a command center or daily flow huddle to monitor systemwide status.
- Measure, adjust, and scale based on pilot outcomes.
For a structured overview of the full methodology, the patient flow management guide provides a detailed framework aligned with current best practices.
Discharge optimization: The highest-ROI patient flow lever
If there is one area where healthcare administrators can generate rapid, measurable throughput gains, it is discharge planning. Discharge is frequently treated as the final step in a patient’s stay, but high-performing systems treat it as a process that begins at admission. That shift in mindset produces dramatic results.
Discharge optimization via early planning and non-peak timing yields 20 to 45% improvements in throughput, according to multidisciplinary research published in 2025. Non-peak discharge scheduling, meaning moving discharges to morning hours rather than clustering them in the afternoon, frees beds during the highest-demand admission windows. This single scheduling adjustment can meaningfully reduce ED boarding time.
| Discharge practice | Impact on throughput |
|---|---|
| Discharge planning initiated at admission | Reduces average LoS by 15-20% |
| Non-peak discharge scheduling | Frees beds during peak admission hours |
| Multidisciplinary discharge rounds | Reduces day-of delays by up to 30% |
| Predictive discharge date communication | Improves patient and family readiness |
Multidisciplinary collaboration is the engine behind effective discharge. When physicians, case managers, social workers, and nursing staff align on a projected discharge date from day one, the entire care team organizes around that target. Streamlining discharge requires clear ownership, shared tools, and daily structured communication.
Pro Tip: Assign a dedicated discharge coordinator to rounds in high-volume units. This role alone can reduce day-of discharge delays by identifying and resolving barriers, such as pending labs or transportation gaps, before they stall the process.
Key actions for discharge improvement:
- Set a projected discharge date within 24 hours of admission.
- Conduct daily multidisciplinary rounds focused on discharge readiness.
- Identify and resolve flow bottlenecks such as pending orders or transport coordination before noon.
- Communicate discharge timelines clearly to patients and families to reduce last-minute resistance.
- Track time-to-discharge as a core operational metric alongside LoS.
Harnessing technology and analytics for proactive flow management
Technology does not fix broken processes, but it dramatically accelerates the performance of well-designed ones. The most significant advances in patient flow management over the past three years have come from AI-powered command centers and predictive analytics in healthcare, which shift operations from reactive to anticipatory.
Digital command centers aggregate data from EHR systems, bed management platforms, staffing tools, and patient tracking systems into a single operational view. Administrators and charge nurses can see projected surges, flag at-risk discharges, and reallocate resources before a bottleneck forms. The results from early adopters are striking.
“AI and predictive analytics, combined with a digital command center, produced a 37% faster admission-to-bed time and a greater than 50% reduction in patients not seen by a provider (NSA patients) within target timeframes.”
These outcomes are not outliers. They reflect what becomes possible when real-time data replaces institutional intuition as the basis for capacity decisions. Key capabilities that drive these results include:
- Surge prediction: AI models forecast patient volume by hour, day, and season, enabling proactive staffing and bed allocation.
- Automated alerts: Staff receive real-time notifications when discharge delays, bed holds, or transport gaps threaten flow.
- Cross-unit visibility: Command centers surface bottlenecks across the full care continuum, not just within individual departments.
- Integration with transport and logistics: Coordinating patient movement, including non-emergency medical transport, within the same platform eliminates handoff gaps.
Piloting technology in a single high-volume unit before scaling system-wide reduces implementation risk and builds staff confidence. Human oversight remains essential. Technology surfaces the data; experienced clinicians and administrators make the calls.
Sustaining improvements: Change management, culture, and surge preparedness
Process redesign and technology investment produce results in the short term. Sustaining those results over years requires something harder to measure: organizational culture aligned around flow as a shared responsibility. Multidisciplinary teams, change management, and surge planning are essential for lasting results, and organizations that skip this layer consistently see gains erode within 12 to 18 months.
Staff resistance is the most common reason flow improvement projects stall. When frontline teams perceive new processes or tools as administrative burdens rather than support mechanisms, adoption suffers. Leadership communication, early staff involvement in design, and transparent reporting of results all reduce this resistance significantly.
Cross-training is another underutilized lever. When staff can flex across units during surge events, the organization avoids the rigid capacity constraints that turn manageable volume spikes into crises. Hybrid human-AI models, where technology handles monitoring and alerting while staff retain decision authority, tend to generate the highest adoption rates.
Pro Tip: Establish a monthly flow performance review that includes frontline nurses, case managers, and unit administrators alongside executive leadership. Shared visibility into the same metrics builds collective ownership and accelerates problem-solving.
A structured approach to embedding flow improvement culture:
- Identify internal flow champions in each major unit to lead peer adoption.
- Provide structured training on new processes before technology goes live.
- Report flow metrics transparently at the unit and hospital level monthly.
- Build surge response protocols that are practiced, not just documented.
- Recognize and reward teams that sustain or exceed flow benchmarks.
- Review and refresh protocols annually to incorporate new evidence and operational learning.
Behind the benchmarks: What most flow management articles miss
Most published guidance on patient flow focuses on what to implement. The harder question is why so many well-designed initiatives fail to hold. The answer, in our observation, is almost never the technology or the process design. It is the assumption that flow is a departmental problem rather than a systemwide coordination challenge.
Organizations that sustain patient flow challenges improvements share one characteristic: they treat logistics as infrastructure, not as a series of isolated projects. When discharge planning, transport coordination, bed management, and staffing decisions operate in separate systems with separate owners, gains in one area are routinely offset by delays in another.
The uncomfortable truth is that culture change is not a soft add-on to flow improvement. It is the primary variable. Technology accelerates what culture enables. Without staff alignment, command centers become expensive dashboards that no one acts on. Without leadership commitment, standardized handoffs revert to informal workarounds within weeks of rollout.
Leading organizations invest as much in communication, training, and accountability structures as they do in platform selection. That balance is what separates organizations that publish benchmark results from those that quietly abandon their flow initiatives after the pilot phase.
Take patient flow management from knowledge to action
The strategies outlined here represent a proven path from operational fragmentation to coordinated, efficient patient logistics. Translating that path into practice requires tools built for the complexity of modern healthcare delivery.
VectorCare’s platform is designed to support exactly this kind of systemwide coordination. From understanding patient logistics fundamentals to maximizing efficiencies across transport, discharge, and home health transitions, the platform gives administrators real-time visibility and automation where it matters most. If your organization is ready to move beyond isolated improvements and build a scalable flow management infrastructure, explore what the VectorCare platform can do for your operations.
Frequently asked questions
What is the best first step for improving patient flow?
Begin with a multidisciplinary review to map current bottlenecks, then pilot changes in high-impact areas like discharge or ED admission before scaling organization-wide.
How much can effective patient flow management reduce hospital wait times?
Structured interventions consistently produce 25 to 38% reductions in patient wait times and length of stay across North American health systems.
Which technology has the most impact on patient flow?
AI-powered command centers and predictive analytics deliver the largest measurable improvements by enabling real-time, hospital-wide capacity coordination and proactive surge management.
How do multidisciplinary teams improve patient flow?
Collaborative teams address process gaps across departments simultaneously, which improves communication and helps sustain efficiency gains that single-department efforts rarely achieve on their own.
Why do patient flow improvement projects often stall?
Most stall due to staff resistance, siloed operations, and insufficient change management investment, not because the underlying process or technology was flawed.
Recommended
- How to Reduce Patient Wait Times Effectively
- Patient Flow Barriers: Impact to Hospital Efficiency and Patient Outcomes | VectorCare
- 6 Ways to Improve Patient Flow Within Healthcare Facilities | VectorCare
- What Is Patient Flow Management? Guide for Healthcare 2025
- Discover how AI and automation are transforming small clinics into efficient, profitable, and patient-focused practices. Learn practical ways to reduce no-shows, save hours each week, and grow without hiring more staff — all explained in clear, actionable steps designed for real clinic owners.