Home health coordination: improving patient logistics in 2026

Hospital-to-home health visit delays have increased despite growing demand and budgets, creating a pressing challenge for healthcare administrators. Coordinating care across multidisciplinary teams and complex logistics is critical for patient outcomes, yet fragmentation and inefficiencies persist. This guide clarifies modern methods and technology solutions to help administrators improve coordination and efficiency. You’ll discover actionable strategies for optimizing patient logistics, reducing readmissions, and meeting regulatory benchmarks while enhancing operational margins through proven best practices and advanced platforms.
Table of Contents
- What Is Home Health Coordination And Why It Matters
- Core Methodologies And Technology In Home Health Coordination
- Operational Benchmarks And Challenges In U.S. Home Health Coordination
- Applying Technology And Best Practices To Optimize Home Health Coordination
- Enhance Your Home Health Coordination With VectorCare
Key takeaways
| Point | Details |
|---|---|
| Interdisciplinary planning | Home health coordination requires dynamic teams and regular care plan reviews for optimal outcomes. |
| Timeliness benchmark | Target less than 3 days from discharge to first visit to meet efficiency standards. |
| Technology integration | AI scheduling and EHR systems improve communication and reduce logistics delays significantly. |
| Medicare distinctions | Medicare Advantage and traditional Medicare have distinct impacts on resource use and patient outcomes. |
| Edge case management | Addressing complex transitions and rural access improves quality and reduces readmissions. |
What is home health coordination and why it matters
Home health coordination involves deliberately organizing patient care activities, sharing information among providers, and creating comprehensive care plans using interdisciplinary teams including nurses, therapists, physicians, and social workers. These teams work collaboratively to address patient needs holistically, ensuring seamless transitions from hospital to home and continuous monitoring throughout the care episode. Each team member brings specialized expertise that contributes to a patient-centered approach focused on recovery, independence, and quality of life.
Key team members include:
- Registered nurses who assess patient conditions and coordinate clinical services
- Physical and occupational therapists who design rehabilitation programs
- Physicians who oversee medical treatment plans and authorize services
- Social workers who address psychosocial needs and connect patients with community resources
- Home health aides who provide personal care and support daily living activities
Care plans are centered on individual patient needs and involve continuous collaboration across all providers. Proper coordination directly impacts patient outcomes by reducing hospital readmissions, improving functional independence, and ensuring medication adherence. When coordination breaks down, patients face gaps in care, conflicting instructions, and preventable complications that drive up costs and diminish satisfaction.
Leadership buy-in is essential to manage fragmentation and compliance challenges effectively. Without executive support, coordination efforts remain siloed and technology investments fail to deliver expected returns. Administrators must champion integrated workflows, allocate resources for staff training, and establish clear accountability structures. Understanding health home care coordination requires recognizing that successful programs balance clinical excellence with operational efficiency, creating systems where information flows seamlessly and every team member understands their role in the patient’s journey.
Core methodologies and technology in home health coordination
Dynamic plans of care reviewed every 60 days or sooner ensure responsiveness to changing patient conditions and evolving needs. These living documents incorporate input from all team members and adjust goals based on progress assessments. Initial and ongoing comprehensive patient assessments set measurable goals for reducing readmissions and improving independence, providing clear benchmarks for success.
Key methodologies include:
- Comprehensive initial assessments that establish baseline functional status and identify risk factors
- Regular interdisciplinary team meetings to review progress and adjust interventions
- Standardized communication protocols ensuring consistent information sharing across providers
- Evidence-based clinical pathways tailored to common diagnoses and patient populations
- Outcome measurement systems tracking quality indicators and patient satisfaction
Technology tools such as EHR systems, AI scheduling platforms, and secure messaging enable seamless information sharing across care settings. Real-time data sharing optimizes logistics by matching patient needs with available resources, reducing delays between referral and service initiation. Patient care coordination tips emphasize that technology should enhance human judgment rather than replace it, providing decision support while preserving clinical autonomy.
Advanced platforms integrate multiple functions into unified workflows. Technology transforming patient logistics demonstrates how AI-driven scheduling algorithms account for clinician availability, patient location, skill requirements, and visit duration to create optimized routes. These systems reduce travel time, increase visit capacity, and improve work-life balance for field staff.
Pro Tip: Implement scheduler protocols that broadcast unplaced cases widely across your provider network rather than assigning them sequentially. This approach reduces unplaced services by 40% and improves compliance with timeliness benchmarks by engaging multiple potential responders simultaneously.
Operational benchmarks and challenges in U.S. home health coordination
Timeliness metrics reveal growing challenges in post-acute transitions. Average days from discharge increased from 2.3 to 2.4 days in 2019 to 3.2 to 3.3 days in 2024Q2, exceeding the target benchmark of under 3 days. This deterioration occurs despite increased awareness of the importance of rapid home health initiation for preventing readmissions.
In 2023, 2.7 million Medicare FFS beneficiaries used home health services, generating $15.7 billion in spending with agencies maintaining 20.2% margins. These figures demonstrate the sector’s scale and financial viability, yet operational inefficiencies continue to constrain growth and quality improvement efforts.
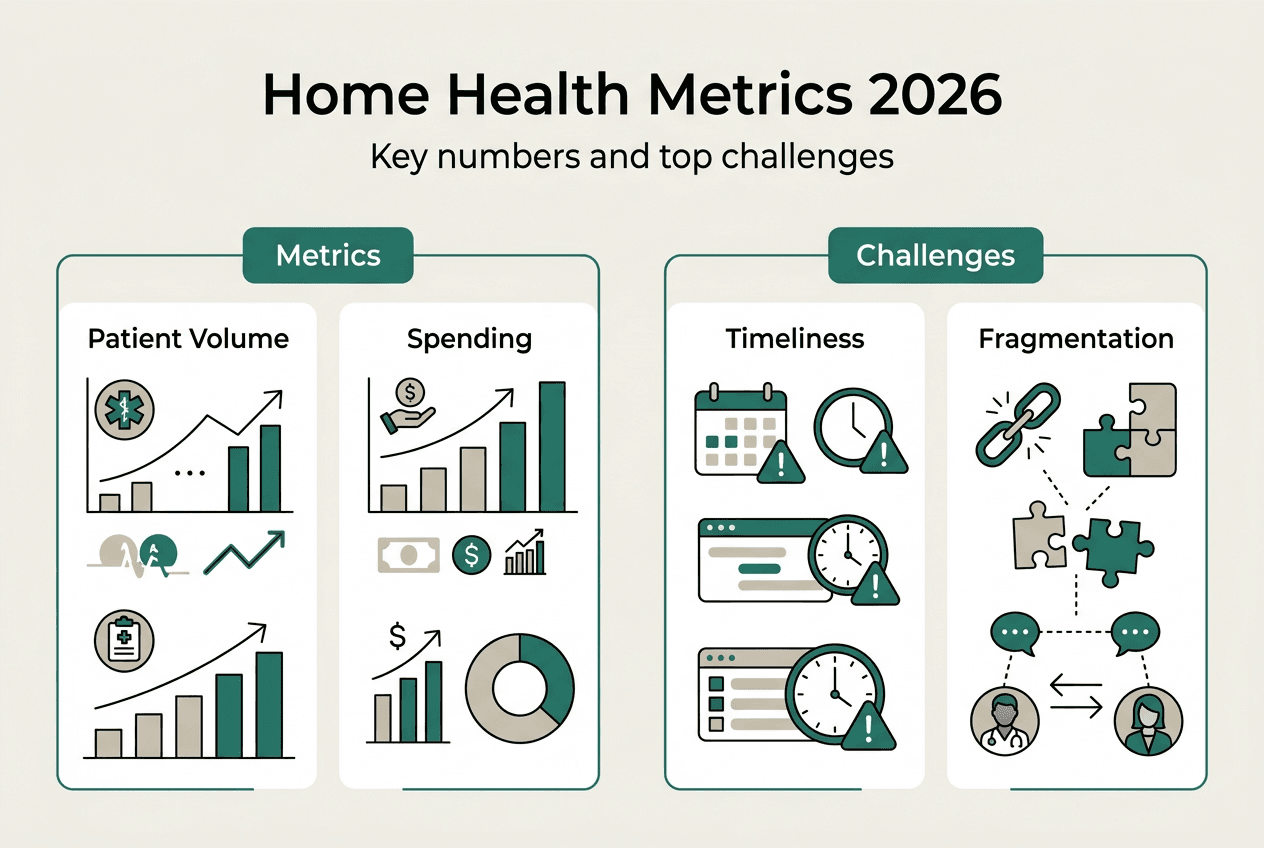
| Metric | 2019 Baseline | 2024 Q2 Current | Target | | — | — | — | | Days to first visit | 2.3 to 2.4 | 3.2 to 3.3 | Under 3.0 | | Medicare beneficiaries served | 2.5M | 2.7M | Growing | | Agency margins | 18.5% | 20.2% | Sustainable |
Edge cases include medically intensive patients and transitions with 55% reported quality issues, particularly in rural areas with limited provider access. These complex situations require enhanced coordination strategies involving social workers, specialized nursing skills, and flexible scheduling to accommodate unpredictable needs.
Medicare Advantage enrollees experience different care patterns than traditional Medicare beneficiaries. Per-visit MA has 12% higher transfers to inpatient settings, while episodic MA yields better outcomes with 34% spending savings from Independence at Home demonstrations. These distinctions matter for administrators managing mixed payer populations who must tailor coordination strategies to reimbursement structures.
Fragmentation and staff burnout challenge coordination efforts across the industry. Clinicians juggle multiple communication platforms, duplicate documentation in disconnected systems, and struggle to obtain timely information from hospitals and physicians. Improving outcomes for Medicare Advantage members requires addressing these systemic issues through technology and centralized leadership that establishes clear workflows and accountability.
Pro Tip: Assign dedicated transition coordinators who own the discharge-to-first-visit process end to end. This single point of accountability reduces handoff failures and ensures no patient falls through the cracks during the critical 72-hour window post-discharge. Tackling discharge delays with technology provides implementation frameworks for this approach.
Applying technology and best practices to optimize home health coordination
Administrators should prioritize interoperable tech including AI scheduling and EHR integration to create seamless communication pathways. Target under 3 days for post-discharge starts and address edge cases with interdisciplinary plans involving social work for complex needs. These foundational practices establish the infrastructure for sustained quality improvement.
Centralizing coordinators at headquarters for information sharing while embedding them in practices balances trade-offs and improves quality metrics. The centralized model ensures consistent protocols and knowledge sharing, while embedded staff maintain relationships with referral sources and understand local market dynamics. Hybrid approaches combining both strategies often deliver optimal results.
Key implementation strategies:
- Deploy unified platforms that eliminate duplicate data entry and provide single-source-of-truth patient records
- Establish real-time visibility into clinician schedules, availability, and current location for dynamic dispatch
- Implement automated alerts for care plan deviations, missed visits, or emerging clinical concerns
- Create standardized templates for common diagnoses that accelerate care plan development
- Build analytics dashboards tracking timeliness, readmissions, and OASIS-E compliance in real time
Use OASIS-E process measures to monitor compliance and outcomes actively. These standardized assessments provide comparable data across agencies and identify improvement opportunities. Apply broadcast scheduling protocols to reduce unplaced cases by engaging your entire provider network simultaneously rather than sequential assignment.
| Approach | Advantages | Best Use Case |
|---|---|---|
| Centralized coordination | Consistent protocols, knowledge sharing | Large agencies, multiple markets |
| Embedded coordination | Strong referral relationships, local expertise | Single-market agencies, hospital partnerships |
| Hybrid model | Balances consistency with local responsiveness | Growing agencies, diverse geographies |
The home health logistics platform from VectorCare integrates these capabilities into a unified system designed specifically for post-acute care coordination. Home health scheduling apps optimize field staff productivity while maintaining clinical quality and patient preferences. Modernizing healthcare dispatching enables value-based care models by providing the visibility and control necessary for population health management.
Pro Tip: Prioritize leadership buy-in and comprehensive staff training when deploying new technology to overcome fragmentation and burnout. Successful implementations involve clinicians in design decisions, provide hands-on training with realistic scenarios, and establish super-users who support peers during the transition period. Technology alone cannot fix broken processes, but the right tools combined with change management create transformative results.
Enhance your home health coordination with VectorCare
Modern home health agencies need more than basic scheduling tools to compete in 2026’s complex post-acute landscape. VectorCare offers a comprehensive patient logistics platform designed specifically for home health agencies facing coordination challenges.
Our platform features AI-driven scheduling that optimizes routes and matches patient needs with clinician skills automatically. Dispatch optimization reduces travel time by 30% while improving first-visit timeliness. Real-time communication tools connect field staff, coordinators, and referral sources in HIPAA-compliant channels that eliminate phone tag and documentation gaps. These capabilities help reduce discharge delays, enhance care coordination, and improve operational margins through measurable efficiency gains. Maximizing patient logistics efficiencies demonstrates how leading agencies achieve 25% productivity improvements and 40% reductions in unplaced cases. Join organizations adopting the VectorCare Hub to modernize healthcare dispatching and boost patient outcomes. Our home health logistics platform provides the visibility and control you need to excel in value-based contracts while maintaining clinical excellence.
FAQ
What is the role of interdisciplinary teams in home health coordination?
Interdisciplinary teams combine diverse clinical expertise to address patient needs comprehensively, ensuring holistic care and seamless communication across all providers. Nurses, therapists, physicians, social workers, and aides contribute specialized knowledge that creates patient-centered plans addressing medical, functional, and psychosocial dimensions. Understanding these team roles is essential for administrators building effective coordination programs.
How frequently should plans of care be updated in home health settings?
Plans of care must be reviewed at least every 60 days or more frequently if patient conditions change significantly. Regular updates ensure responsiveness to evolving needs and maintain compliance with Medicare Conditions of Participation. Many high-performing agencies conduct informal reviews weekly during interdisciplinary meetings to catch emerging issues early.
What technology tools best support effective home health coordination?
EHR integration ensures comprehensive, accessible patient records across all providers involved in care. Secure messaging enables quick, HIPAA-compliant communication that eliminates delays from phone tag. AI-driven scheduling optimizes resource use and reduces delays by matching patient needs with clinician availability and skills automatically. Home health scheduling apps and technology transforming patient logistics provide concrete examples of these tools in action.
What key metrics should agencies track to measure home health coordination success?
Tracking days from discharge to first home visit targets efficiency goals, with best practice benchmarks under 3 days. Monitoring readmission rates within 30 and 60 days reflects care quality and coordination effectiveness. OASIS-E compliance measures demonstrate regulatory adherence and identify opportunities for patient outcome improvement. Tackling discharge delays shows how leading agencies use these metrics to drive continuous improvement and competitive advantage.
Recommended
- Top Patient Care Coordination Tips for Better Outcomes
- Ambulance Providers as Patient Logistics Centers | VectorCare
- How Technology is Transforming Patient Logistics for SNFs | VectorCare
- Maximizing Efficiencies Through Better Patient Logistics | VectorCare
- Role of Home Rehabilitation – Transforming Stroke Recovery